On July 24, 2020, Indiana governor Eric Holcomb signed executive order 20-37 requiring that face masks be worn in public to halt the spread of COVID-19. The statewide mandate was based on recommendations from the Centers for Disease Control, the Indiana State Department of Health, and other public health authorities. Since its inception the original mandate has been extended 5 times in 2020. The figure below shows the relationship between the original mask mandate, its extensions, and the number of new cases of COVID-19 in Indiana:
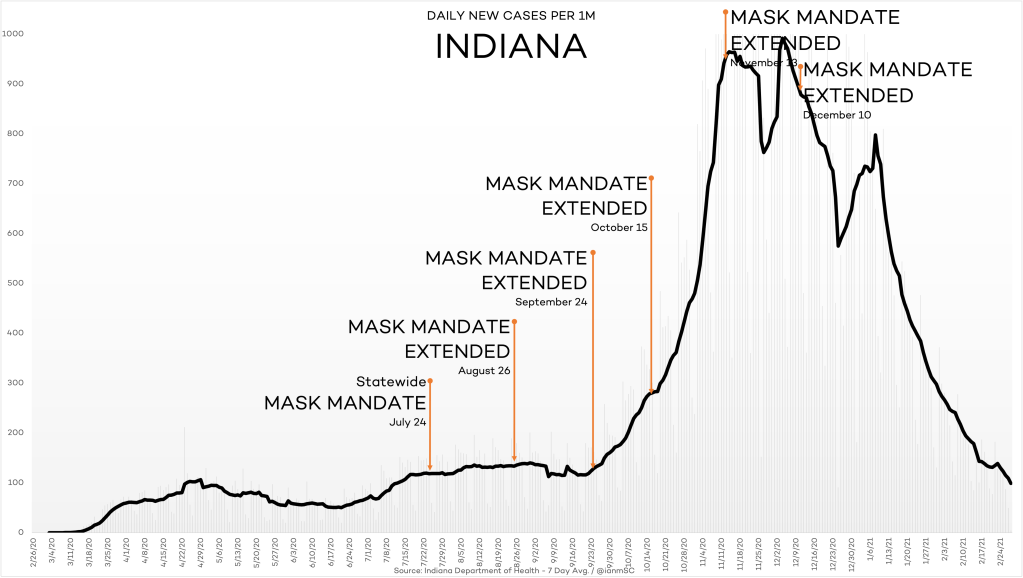
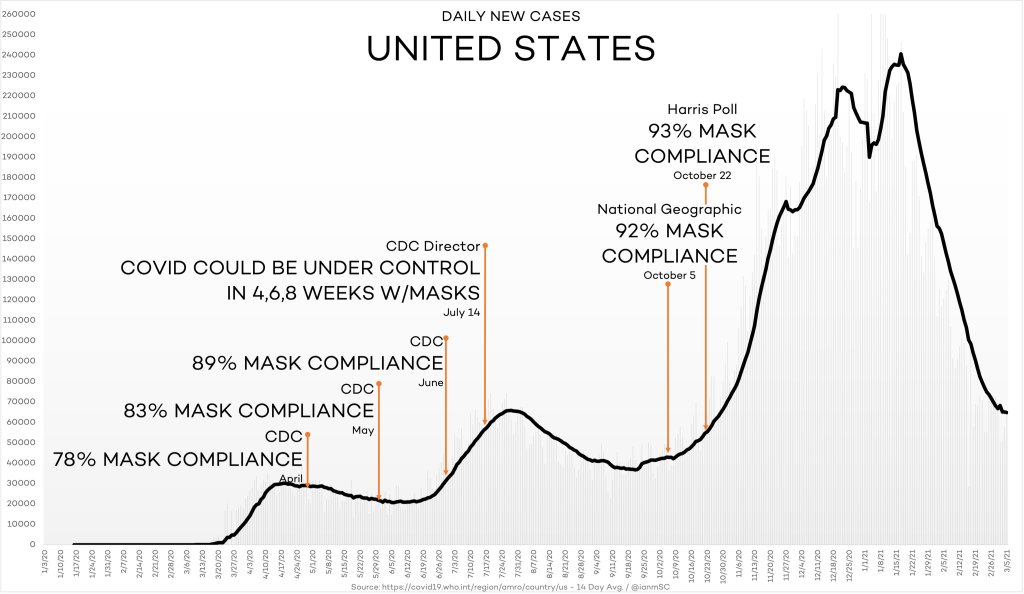
What is apparent is the lack of any discernible relationship between the mask mandate and rise in new cases. A similar pattern is observed nationally despite almost 100% self-described compliance with face mask use by Fall 2020:
We have been assured repeatedly by our most authoritative public health institutions and leaders that masking is an essential mitigation strategy that confers protection against COVID-19. To better understand why mask mandates do not seem to influence case numbers we need to closely examine the best available scientific evidence on face masks. Doing so in an impartial manner leads to only one conclusion: that face masks in a community setting offer no protection against respiratory viruses, including COVID-19, for the wearer or others nearby (e.g. household members).
Scientists, physicians and epidemiologists are taught early in their careers that randomized controlled trials offer the best quality scientific evidence because of their gold standard study design. It is therefore critical to focus on the results of these types of studies. Ten randomized controlled trials, all published between 2008 and 2016, have in a variety of community settings examined whether face masks reduce the risk of laboratory-confirmed influenza. None found face masks to have any protective benefit either for the wearer or others in close contact with the wearer. In May 2020 the Center for Disease Control’s own journal Emerging Infectious Diseases published a report that reanalyzed these ten studies by pooling their data to exclude the possibility that each study was too small on its own to see a statistical difference. Still no benefit of face masks was observed.
There have subsequently been two additional randomized controlled trials of face masks, each larger than all the ten original studies combined. The first was performed in the pre-COVID-19 era, published in 2020, and reported that face mask use in 7687 pilgrims to Mecca did not protect against viral respiratory infections. The second study, published in November 2020, is the only existing randomized controlled trial that specifically addressed face masking for COVID-19. Completed in Denmark, a nation that never enforced face mask usage during the pandemic, this unique trial in 6024 individuals found that surgical face masks worn in the community did not protect the wearer from COVID-19. Limiting the analysis to the participants who reported wearing masks “exactly as instructed” did not change the result. Since every existing randomized controlled trial on face masks has concluded that they are not effective against respiratory viruses like COVID-19, it should come as no surprise that the mask mandate in Indiana did not seem to control the rise in new cases. In fact, the negative trial data simply confirm public health experience gained a century ago on the lack of efficacy of face masks in protecting against another infamous respiratory virus, the Spanish Flu. What the curve of new cases in Indiana shown above in all likelihood represents is the known seasonality of respiratory viruses like COVID-19 and/or the development of population (i.e. herd) immunity as it spread through the Hoosier state.
There will be individuals who dismiss these findings, arguing that since wearing masks is only a slight inconvenience we are obligated to do so both as a public expression of concern for others as well as to “hedge our bet” in case the randomized trial data are all wrong. I respectfully disagree with this position on several grounds. First, there is the principle of the matter. We are either a society that develops public health policies based on rigorous scientific methods, or we are not. If the latter then we need to drop any pretense that our public health care is based on a scientifically rigorous, reality-based approach. Second, describing masks as a minor inconvenience greatly downplays the negative impact they have on impairing normal human communication and interaction and making breathing more difficult. Masks also encourage the counterproductive effects of giving people a false sense of security about the virus and promoting touching of masks and faces, all of which could theoretically increase viral spread. Moreover, there are potential risks that we haven’t begun to seriously consider, such as the impact of constant inhalation of microfibrils into the lungs from face masks of all types, or even others that have not yet occurred to us. Finally, the damage face masks have done to impair the social and psychological health of our children should be of great societal concern. One example is that for the first time in history we now have a population of infants who for their entire livespan have seen only the unmasked faces of their immediate family members. This is akin to an unprecedented society-wide experiment on childhood development that has bypassed any type of informed consent.
Fifteen states have now lifted their mask mandates based on at least some of the issues I have raised. Unfortunately, Indiana is not one of them. It is therefore high time for Indiana to join these states and immediately lift its mask mandate. By doing so, it will demonstrate good public policy from the standpoint of evidence-based science and the overall well-being of its citizenry.
